

Pill or Prevention?
The Case for Both
“Let food be your medicine” has been a common saying for ages. Can our desire for “natural” solutions to our health concerns be balanced with a thoughtful application of modern pharmacology?












No one doubts the necessity of prescription drugs. Well, almost no one. There are certainly those who believe the human body is such a wonder that not keeping it as natural as possible is our greatest failing, maybe even a driver of disease.
At their extreme, these nature-only folks can be easy targets. Elizabeth Nolan Brown, senior editor at Reason magazine, disparages the cast of characters in today’s natural health movement as “protein-maxxing health bros, raw milk–drinking trad wives, toxin-fearing food babes, vaccine-critical Insta moms, tallow-promoting beauty vloggers, and all sorts of other body-as-temple types [who] sell new solutions, provide new scapegoats, and offer . . . new ideas about what it means to live virtuously.” A few critics of modern medicine have gone even further, claiming that germs don’t really exist; rather than infections being caused by invasions of microbes from outside our bodies, our troubles are due to imbalances within.
Ulric Williams (1890–1971), a proponent of an alternative health system called “terrain therapy,” boldly asserted that right food (among other good habits) was the better cure, not medicine. “For too long we have thought like idiots, fed like fools, and acted like knaves; and then swallowed poisons or had pieces cut out of us in the hope of ridding ourselves of the consequences.”
It’s a striking observation—and Williams wasn’t wrong in that how we live clearly matters. But the question isn’t whether to trust nature or science. It’s how to draw wisely from both.
Unfortunately, as in many areas of human concern and opinion, we are becoming polarized in our thinking about health. Are we walking only the path of medicalization—seeking a pill for every malady while ignoring how we live, think and eat? Or are we traveling to the opposite extreme: shunning medical therapies as unnatural and more toxic than therapeutic? Where is complementarity, the sweet spot where the right use of medicine and a right understanding of the body’s capacity to ward off disease and heal itself overlap?
The Biomedical Model
The body is a wonder. Still, most welcome and embrace the interventions of modern medicine and the orthodoxy of antibiotics, vaccines and other drugs. These curatives work because, first, germ theory holds true. Pasteur was right: Sewage-tainted rivers should be avoided. Clean water is important. And second, we have developed a good understanding of how the body works chemically.
This is the biomedical model of health. Discovering the physiology of disease and creating drugs to alleviate or counter specific malfunctions has served us well. After all, we are living longer than at any time in our recorded history, and this can be attributed in large part to controlling infections and curtailing other diseases through drug-based therapies.
But this model is not perfect. Preventive behaviors have also contributed to longer, healthier lives. So while germ theory does account for infections, how we live and eat, and the environment we are exposed to, also matter; it’s not “one or,” it’s “one and.” If there’s an error with modern medicine, it’s the tendency to attribute singular causes and prescribe singular solutions for complex ailments. Behavioral scientist Evan G. Pattishall (1921–2003) put it this way: “We seem to operate with the blind hope that we will somehow be able to understand the human being if we can only isolate the smallest component parts. We have settled for an understanding of the mechanics rather than the process; the single variable rather than the multivariable; the isolated parts rather than the integrated whole; irrelevancy rather than meaning.”
The problem is generally not that drugs don’t work but that the way they are developed, tested and delivered can sometimes undermine public confidence in them. Science isn’t a debate where the most appealing hypothesis wins; reliability and credibility rest in the data. But that doesn’t mean science and scientists don’t make mistakes. And, because drug development is a business, considerations of profit and market can corrupt the data or its interpretation.
Jerry Avorn is a professor of medicine at Harvard’s Brigham and Women’s Hospital. In 1998, he founded the Division of Pharmacoepidemiology and Pharmacoeconomics to improve our understanding of drug effectiveness, necessity, side effects and cost. In Rethinking Medications: Truth, Power, and the Drugs You Take, he reports that although we have gained incredible insight into the biology of disease, we have not always done a good job of delivering these insights: “Our remarkable scientific victories have not been accompanied by comparable advances in getting such discoveries to those who need them, or in doing enough to ensure the effectiveness, safety, and affordability of the medications that people take.”
Avorn explains that pharmacoepidemiology is the study of “what goes right and goes wrong after molecules leave the lab and make their journey into people’s bodies. Sometimes the path is swift and direct and leads to excellent results. But other times it takes unexpected turns that can produce awful outcomes.” So, no matter where we happen to live, his analysis is “directly relevant to anyone who takes or prescribes a medicine or cares about someone who does, as well as to anyone who pays taxes or health insurance premiums.”
“I encourage skepticism. I don’t think anyone should just go into a doctor’s office and say ‘yes, yes, yes, yes.’ In fact, I love when my patients question me. . . . If you Googled, and you have questions, now I know exactly the route I need to take to help you make a decision that’s right for you and your family.”
As Avorn suggests, “Understanding this pathway can shed light on what drugs people should take or might want to question, and what needs to happen in the doctor’s office.”
An important part of that pathway is the research that underlies the invention and development of the drug itself. A troubling artifact of drug development is the allowance for companies to design and administer their own efficacy trials. Results incompatible with research or marketing goals can sometimes be suppressed. Such practices erode trust, not only in the drugs but in medicine itself. (See “The Drug Business,” below.)
Recognizing that errors (even egregious or illegal ones) occur doesn’t mean that we should lose sight of the basic value of medications or the biological foundations they’re built on. Other models of care, such as terrain therapy, have laudable goals and provide some important insights (such as the need to take care of your body), but the reasoning underlying them may, in some cases, lack scientific support.
A Mistaken Observation
In terrain therapy, which originated in 19th-century France as a counterpoint to Louis Pasteur’s work, bacteria and viruses are considered symptoms rather than causes: they were believed to form and grow within the body as a result of disease. In this view, how we conduct our lives and treat our bodies—the terrain—is of the highest importance. But since exterior bacteria are harmless in this view, does that mean swimming in sewage-contaminated rivers is okay after all?
Terrain therapy seems quite useful when only considering its goal of a body in healthy equilibrium. But a deeper dive into terrain theory reveals flawed foundations that don’t support its explanations and teachings.
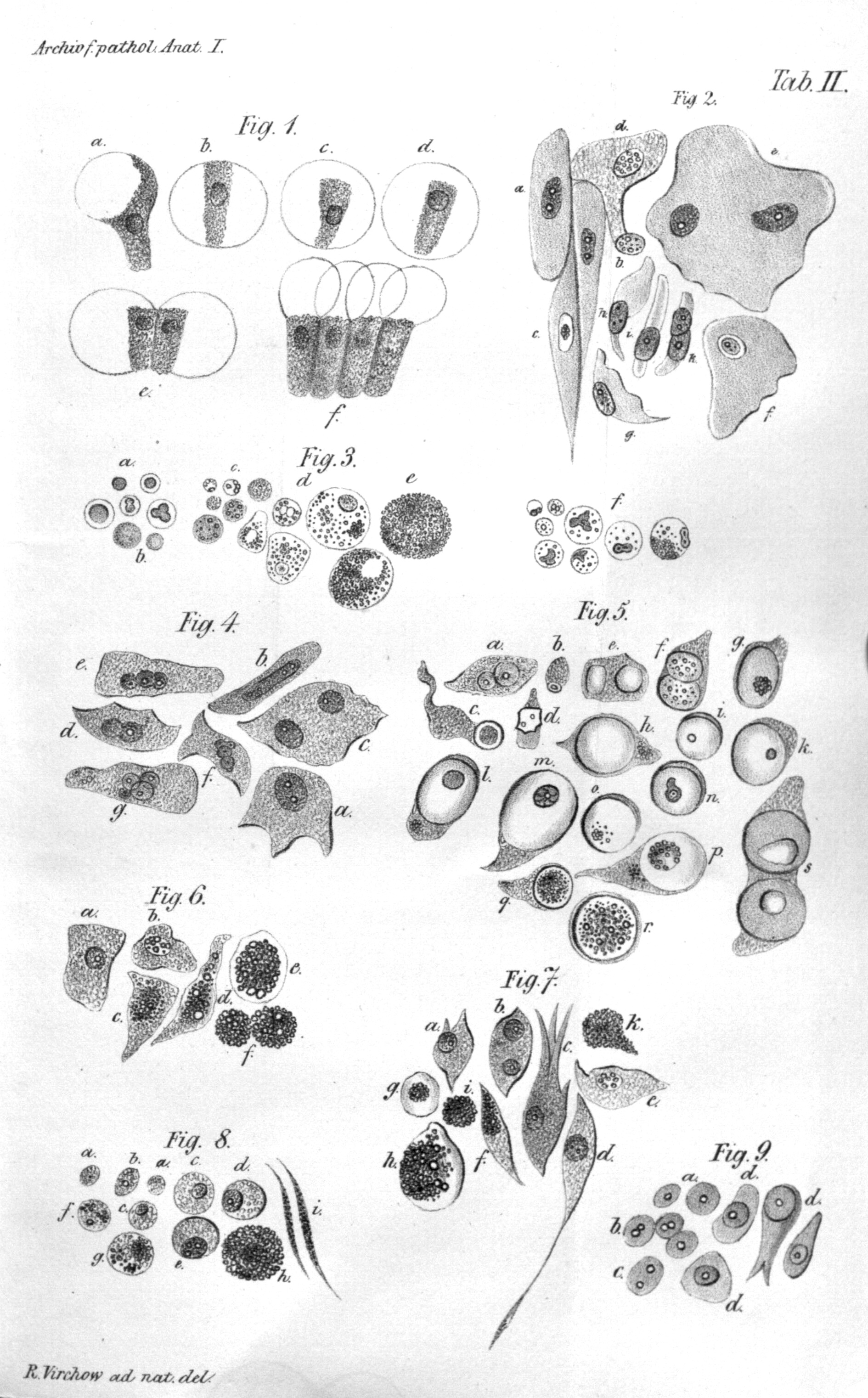
The theory arose when Pierre Antoine Bechamp proposed his own theory of disease. At that time bacteria and fungi were known to be associated with fermentation and decay, and the origin of these microbes was still being debated. Bechamp’s solution was previously unknown particles he called microzymas, which he believed were the indestructible essence of life. “They function in each cell, organ, and anatomical system, naturally, chemically and physiologically for themselves, while preserving their individuality,” he wrote. He believed they were the particles being visualized as “stipples” in the contemporary cell diagrams. Today we would describe this as the cytoplasm of the cell—the fluid and structures we now recognize as ordinary cellular components, such as ribosomes, vacuoles and the like.
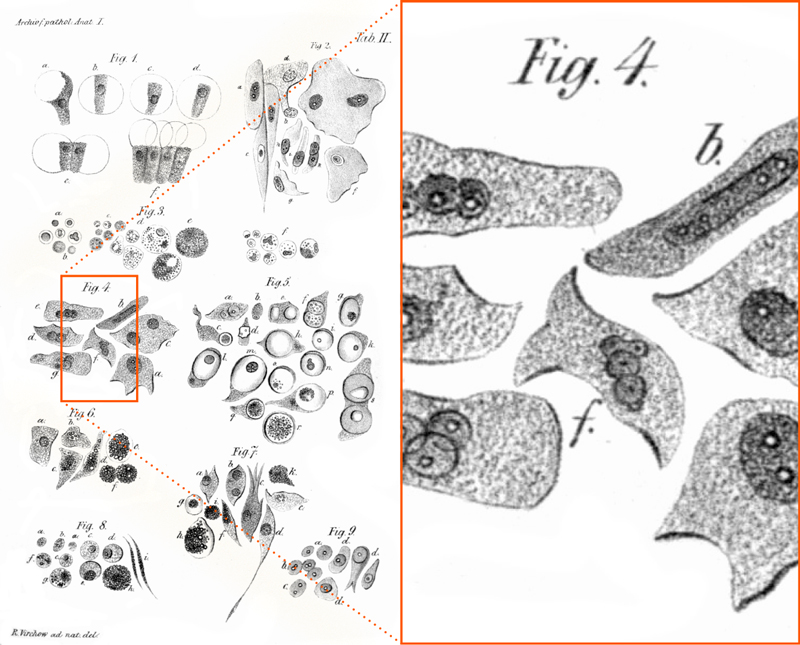
This drawing of different types of cells (left) illustrates the state of the art in 1847. Microscopes had low resolution; photographic analysis did not exist. What we call cytoplasm today was drawn as mysterious granules (see the enlargement on the right). Bechamp incorrectly believed that these stipples revealed the secret of life: life-giving microzymas.
Source: Wikimedia Commons
{kind=link}
Bechamp believed the microzymas directed the making of proteins and the cell itself. When the body was disrupted, he argued, the microzymas became dysregulated and evolved into bacteria, which then produced the diseased state. Therefore, he concluded, “the cause of our diseased condition is always within ourselves. External causes contribute to the development of the affliction and hence of the disease only because they have brought about some material modification of the medium in which live the ultimate particles of the organised matter which constitutes us—namely, the microzymas.”
“People with clean systems [bodily functions] are naturally immune; but disease germs, having appeared in the unhealthy, may disseminate disease among any whom unhealthy living has rendered susceptible.”
Almost 200 years later we know that this narrative is false—clever and intriguing, but incorrect. The development of antibiotics, for example, has been a lifesaver, not a menace to the body. Nevertheless, naturopath Herbert Shelton (1885–1985) proposed an alternative treatment scheme called Natural Hygiene. Insisting that “all medicine is poison,” Shelton argued that it was the adulteration of the purity of the body that led to disease. “What is the real objective of the Hygienic movement? . . . Hygiene must destroy, root and branch, the whole drug system and give to the people a system of mind‐body care that is based on the laws of nature.”
These ideas and more modernized versions of them continue to proliferate online. One purveyor of terrain therapy–like advice and supplements was sanctioned by the Federal Food and Drug Administration in the United States in 2020 for offering unorthodox COVID-19 cures. The FDA warned him to “review all other claims for your products and services and immediately cease making claims that are not supported by competent and reliable scientific evidence.” It’s a good idea for all of us to do the same when faced with extravagant drug promises, be it online or in a doctor’s office. The appeal of natural cures is understandable. But if the pursuit of nature rejects evidence outright, it becomes not restorative but reckless.
That said, scientifically sound natural treatments and cures do exist. And when prescribed by properly licensed practitioners, they can be invaluable, as can informed self-care. Our bodies are “wonderfully made” (Psalm 139:14), resilient against disease, though decidedly less so when subjected to poor nutrition, mental stress and environmental pollutants.

Complementarity
Some still echo the Pattishall warning of decades ago. Simply finding a drug to shift a biomarker (such as an ACE inhibitor to reduce blood pressure) doesn’t get to the heart of the problem: Why is the blood pressure high in the first place? If medicine still operated according to that paradigm, critics would be correct. But the medical community has corrected course. Today it’s clear that both paths can be helpful: a drug-centric therapy as well as behavioral change that speaks to upstream causes. We’ve come a long way in understanding the “integrated whole” and its relationship to health. Very few doctors today would suggest “Just take this pill and call me in the morning,” imagining that was the end of the health maintenance story.
As one research report notes, “following the increased awareness of the importance of lifestyle for disease prevention, we are now facing a renaissance of nutrition, or lifestyle in general, for disease management as well. In this context, disease management not only comprises lifestyle interventions to improve general health and well-being of patients, but also nutritional strategies to stabilize or even ‘reverse’ the disease process itself.”
If you’re looking for someone to agree with the idea that food can be a kind of medicine, then there you have it; the medical community would agree. What we choose to consume, both mentally and physically, is very important to our overall well-being. But that truth does not negate the value of pharmacology.
“There’s a duality here, not a false dichotomy. It’s not just lifestyle or medication. It’s lifestyle for everyone, and for who benefits—high risk, who needs an added layer—medication is definitely an option.”
There is a common ground; in practice, however, finding it may prove difficult, because the friction between the antidrug, naturopath camp and those with a pharmaceutical alliance is extreme. In Super Agers: An Evidence-Based Approach to Longevity, for example, cardiologist Eric Topol discusses the multivariables of lifestyle in relation to our diseases. Topol is chair of the department of Translational Medicine at Scripps Research. Translational medicine studies how to apply medical data and discovery to patient care.
“When we get into discussions of ‘healthy lifestyle,’ it usually refers to diet, exercise, sleep, and intake of alcohol, coffee, and tobacco,” Topol writes. Because the impactors on our health stretch beyond these common factors, Topol proposes broadening the scope: “My much broader definition, lifestyle+, adds environmental conditions such as exposure to toxins including air pollution, microplastics, forever chemicals, socioeconomic status, loneliness, and social isolation.”
Without a doubt all these factors are substantial contributors to our health status—a list that terrain therapists would agree consists of significant disruptors of bodily balance. Our goal remains to dodge the infections of the near term and, in living longer, to reduce the burdens and diseases of aging: chronic conditions of cancer, diabetes, cardiovascular stress and neurodegenerative decline. In many cases, stepping in with the right therapy—whether a pharmaceutical, a scientifically sound natural therapy, or a change in life habits—can be life-extending or even lifesaving.
“Most people, frankly, are not motivated until they know that there’s a goal: Don’t get this disease, and this will help you not get diseases,” says Topol. That goal might be an important change in a certain biomarker—BP, LDL, CRP or heart rate—that warns of trouble ahead. “And we’re going to get other things to help, not just lifestyle,” Topol adds. The supermarket, pharmacy and gym can all be complementary tools.
Back to Basics
We are intimately attached to our own body and are necessarily deeply interested in its well-being. Will we take action to care for our own health? Karen Hacker, director of the US National Center for Chronic Disease Prevention and Health Promotion, summarizes the position we find ourselves in and the decisions we face: “As we look to the future regarding lifestyle changes, we will be contending with both the challenges to prevention and the opportunities that technological innovation brings. Simultaneously, the burgeoning pharmaceutical options for the treatment of diabetes and obesity, for example, may make prevention less urgent. After all, why focus on environmental changes if treatment is available?” The potential dilemma is increasingly real, and the temptation presented by a seemingly easy fix can be strong.
“Increasing evidence shows that, . . . particularly during the early stages of disease, sustained lifestyle changes are by no means inferior to drug treatment, and often even more efficacious in stabilizing or even reversing the disorder.”
Because of the dire situation some of us may find ourselves in, we may really need a drug right now. But can we also see that the better path is to try to avoid the need altogether? When we have a stronger understanding of where the pharmaceutical industry fails and succeeds, combined with a more finely tuned knowledge of the origin of counterclaims that undercut legitimate medical advice, we are primed to make better health-care choices.
“Without prevention,” Hacker warns, “across the world, we will likely continue to see increases in chronic diseases at younger ages and all the consequent results of growing morbidity and economic consequences. This will also be a challenge to lifestyle medicine given the public’s appetite for easy fixes.”
Sometimes the “easy fix” is the only accessible fix. Sometimes our “terrain” and its exposures are also out of our control. Still, in whatever situation we find ourselves, there are wiser and less wise choices about what to do next: to drug or not to drug?
When it comes to enhancing our health, can food be our medicine? Of course, and so can exercise, and sleep, and community, and friends. An apple a day may help keep the doctor away. But when it doesn’t, a statin or a GLP-1 regulator—when prescribed to the right individual at the right time—might be what keeps you well. Wisdom lies not in choosing between nature and science, but in wisely drawing from both.
The Drug Business
There’s no doubt that pharmaceuticals have greatly enhanced our lifespan, our physical and mental comfort, and our general health over the last century. But modern medical care rests on more than a chemical in a pill or syringe. It depends on honest science in drug testing and trials, physicians unbiased by drug sales reps, and our own ability to understand the costs and benefits of a particular medical regimen.
This framework can break down. Lisa Ratta, a former drug sales rep, warns; “If a physician prescribes you a medication, ask if they are a speaker for that medication or the manufacturer. Ask if they attend all-expenses-paid conferences by a particular company. If they do—run.”
Drugs are products—manufactured, marketed and sold. And sometimes oversold. In Rethinking Medications, Jerry Avorn writes that while companies’ duty to generate profits is supposed to stop short of breaking the law, “if there’s a way to modify the law . . . then that becomes part of a company’s job as well.”
Avorn urges patients to be more proactive, acting on two levels: “the personal—to take a more active role in decisions about one’s own medicines, and the political—to reshape the policies that govern these domains.”
On a personal level, Avorn suggests that for each medication, you do the following:
- Ask the prescriber, “Is this drug for treatment or prevention?
- Ask, “What is the goal of this treatment?”
- Ask, “How will I know when this goal is reached?”
- Ask, “What are the most important side effects?”
- Bring a “brown bag” of all your current medications and supplements—whether prescriptions (from all your doctors), over-the-counter medications, herbal remedies or vitamin/mineral supplements—to your practitioner or pharmacist so synergistic (or drug combination) side effects can be avoided with the new medication. Don’t rely on AI to catch dangerous combinations.